Remote patient monitoring: a technology or a care model?


I recently came across a nice publication describing an example of a real world implementation of remote patient monitoring (RPM) for patients with Covid-19 at the Mayo Clinic. There are a few aspects of this paper that I particularly liked that I will discuss, but it also led me to think about a more fundamental question of whether provider organizations should approach RPM as a set of technologies, or a care model?
RPM refers to digital technologies that allow for the capture of health data from patients remotely (eg. at home) and the transmission of that data to providers in order to guide the diagnosis and management of health conditions. At a high level, the technology is broken down into the following components: hardware that detect the health data (eg. glucometer, blood pressure cuff, scale, pulse oximeter, ECG tracing), software that organizes and at times analyzes the health data, and the capability to transmit the health data and insights to the provider, often via an online portal or integration with an existing system such as the electronic health record (EHR). The value proposition for RPM has mostly centered around disease prevention through early detection and decreasing healthcare utilization, although the Covid-19 pandemic has surfaced the additional benefit of decreasing unnecessary in-person patient/provider interactions, which has greatly accelerated the interest and adoption of RPM.
A frequently noted challenge and barrier to adoption for RPM companies is “integration” into care delivery. The barrier is often seen as technical, with a common one being integration of data from the RPM system into the provider’s EHR. This problem, in fact, is often more easily solved than expected, as there are a variety of methods for integrating external data into EHRs. I believe that a more important question is how RPM integrates with the care model it is meant to improve.
Coffrey et al. describes in the latest issue of npj Digital Medicine a RPM program for managing patients with Covid-19 at the Mayo Clinic. The technology component of the program is fairly simple: a set of equipment provided by Mayo to patients for monitoring vitals signs at home (thermometer, blood pressure cuff, pulse oximeter) that deliver patient reported data to providers via either manual entry or passive collection from bluetooth connected devices.
What caught my attention about this paper was not its RPM technology, but how they presented the RPM implementation as a comprehensive care model. The components of the RPM care models are summarized in this table. The care models were centered on a specific patient population (Covid-19) and detailed in a granular fashion the value added steps needed to deliver care for those patients. The technological component was only a piece of an overall tech enabled process that includes care pathways and care team engagement methods specific to this care model.
This way of presenting a RPM implementation is important because it highlights that the implementation is actually that of a tech-enabled care model rather than just a technology. The endpoints they propose to evaluate the RPM program were also appropriately chosen to capture the processes of this care model.
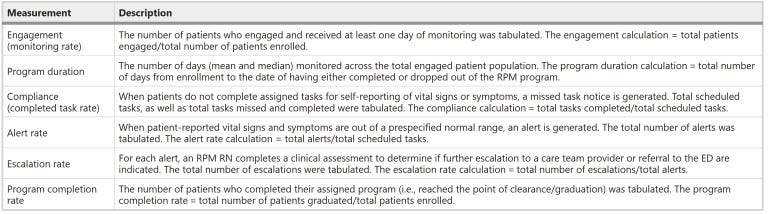
RPM evaluation endpoints (from https://www.nature.com/articles/s41746-021-00490-9/tables/4)
Recognizing what it is that we are actually implementing is critical for understanding the barriers and facilitators to implementation and the expected impact on care delivery. Often, what may initially appear as an implementation of a technology such as RPM is actually an implementation of a new care model. And implementation barriers, such as data integration challenges many RPM companies face with provider organization clients may appear to be technical on the surface, but in reality arise from the lack of a clear RPM enabled care model.
Getting the data in is easy, knowing how to use it is harder.